When families ask about DBS success rates, they almost always get one of two unhelpful answers.
A vague “60 to 80%” with no context. Or a glowing paragraph about life-changing results with no specifics at all.
Neither helps a family decide whether surgery is right for their loved one.
The deep brain stimulation success rate is real, well-documented, and condition-specific. What it means for a 58-year-old with Parkinson’s is different from what it means for a 42-year-old with essential tremor. This article gives you the actual numbers, what they measure, and the honest factors that separate a successful outcome from a disappointing one.
How Deep Brain Stimulation Success Rate Is Actually Measured
Before comparing numbers, it helps to understand what researchers are measuring. “Success” in DBS is not a single definition. Different studies use different measures, and conflating them leads to confusion.
The most common success metrics used in DBS research are:
- Responder rate: percentage of patients achieving more than 50% reduction in their primary symptom (tremor, seizure frequency, or motor score)
- UPDRS-III motor score improvement: the standard clinical rating scale for Parkinson’s motor function; improvement of 30% or more is considered clinically meaningful
- Patient-reported satisfaction: percentage of patients who report the procedure helped them manage their condition
- Medication reduction: reduction in dopaminergic medication dose after DBS, measured as levodopa equivalent daily dose (LEDD)
- Quality of life scores: standardised questionnaires measuring independence, mood, sleep, and daily functioning
A study reporting “75% success” may mean 75% of patients rated the procedure positively. Another reporting “60% success” may mean 60% achieved the clinical threshold for motor score improvement. These are different measures of the same surgery. Understanding which metric is being used matters enormously when evaluating any quoted success rate.
“Families come to me with printed success rate figures from websites and ask me to confirm them. I always start by asking: success as measured by what? Because the answer changes significantly depending on what outcome you are measuring and in which patient population.”
Dr. Jaspreet Singh Randhawa, MCh Neurosurgery (Gold Medalist), Medisyn Neuro Centre, Mohali
DBS Success Rate for Parkinson’s Disease
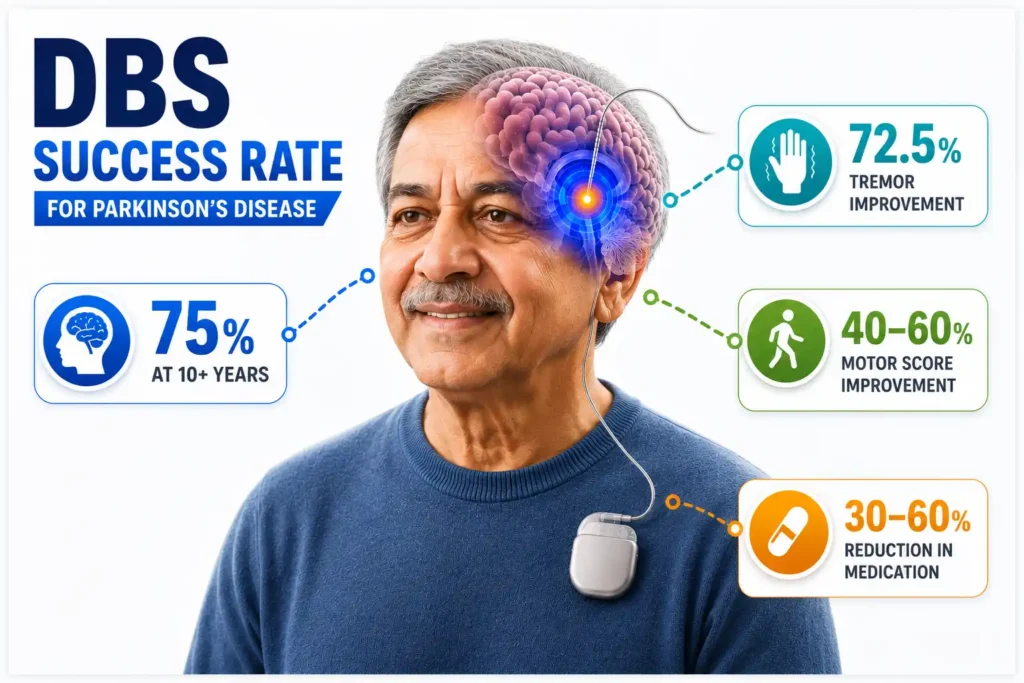
Parkinson’s disease is the most common indication for DBS surgery, accounting for approximately 67% of all procedures globally. It is also the condition with the most long-term outcome data.
Key findings from published research:
- In a 2019 long-term study of 200 Parkinson’s patients followed for over 10 years, 75% reported the procedure helped them manage their symptoms
- A 2025 five-year follow-up study published in JAMA Neurology covering 137 patients found significant improvements in motor function, dyskinesia suppression, and daily living activities sustained across the entire five-year period
- Tremor responds best to DBS in Parkinson’s; in the same 10-year cohort, 72.5% of patients showed tremor improvement
- UPDRS-III motor scores improve by 40 to 60% in appropriately selected patients during optimal stimulation
- Anti-Parkinson medication doses reduce by 30 to 60% in most patients, reducing medication-induced dyskinesias significantly
The honest qualification: DBS for Parkinson’s manages motor symptoms. It does not halt disease progression. Non-motor symptoms including cognitive decline, speech difficulties, and autonomic dysfunction continue their natural course. Patients and families who understand this distinction make better decisions and report higher satisfaction after surgery.
What predicts a strong outcome in Parkinson’s DBS is consistent across all major studies: good levodopa response before surgery, no significant cognitive impairment, correct target selection, and an experienced functional neurosurgeon performing the procedure.
DBS Success Rate for Essential Tremor
Essential tremor is where DBS delivers its most dramatic and consistent results. Of all conditions treated with deep brain stimulation, essential tremor has the highest success rate and the fastest response after device activation.
- Tremor reduction exceeds 90% in most published series for VIM thalamus DBS in essential tremor
- Results are typically seen within days of device activation, unlike Parkinson’s where months of programming are needed
- Bilateral hand tremor can be addressed through bilateral VIM-DBS; unilateral is sufficient when only one hand is affected
- Long-term follow-up data shows sustained tremor control for 10 or more years in the majority of patients
Essential tremor DBS is also more predictable than other indications because the mechanism is straightforward: the VIM nucleus is overactive, and continuous stimulation suppresses that overactivity with high reliability. There is less variability in outcome compared to Parkinson’s or dystonia.
“For essential tremor, DBS is genuinely transformative in a way that is immediately visible. A patient who could not hold a glass of water before surgery can often do so the morning after activation. The family watches it happen in real time. That is why I consider essential tremor the most satisfying DBS indication from a pure outcomes perspective.”
Dr. Jaspreet Singh Randhawa
DBS Success Rate for Dystonia
Dystonia shows the widest range of DBS outcomes of any indication, and understanding why is critical for setting realistic expectations.
| Dystonia Type | Typical DBS Success Rate | Key Factor |
|---|---|---|
| Primary genetic dystonia (DYT1) | 70 to 90% symptom improvement | Best-responding type; no structural brain damage |
| Non-DYT1 primary dystonia | 60 to 75% improvement | Good outcomes; slightly more variable |
| Cervical dystonia (Botox-resistant) | 50 to 70% improvement | Comparable to long-term Botox in responders |
| Tardive dystonia | 60 to 80% improvement | Unusually good response for a secondary cause |
| Secondary dystonia (stroke, CP) | 20 to 40% improvement | Variable; depends on extent of brain damage |
One important difference from Parkinson’s: dystonia DBS benefit is slow. Patients should not judge outcomes at one month post-activation. Full benefit takes three to twelve months as the brain adapts to sustained stimulation. A patient who sees only modest improvement at month two may be a strong responder by month nine.
DBS Success Rate for Drug-Resistant Epilepsy
The SANTE trial, the most rigorous long-term evidence base for ANT-DBS in epilepsy, shows a clear pattern of improving success over time:
- Year 1: 43% of patients achieve more than 50% seizure reduction
- Year 2: 54% responder rate
- Year 5: 68% responder rate
- Year 7: 74% responder rate; median seizure reduction of 75%
This pattern, where efficacy improves the longer the device is in place, is fundamentally different from medication tolerance. DBS for epilepsy does not wear off. It continues working harder over years as the brain adapts to the stimulation pattern.
The most severe seizure type, focal to bilateral tonic-clonic, was reduced by 71% at seven years. This directly reduces the risk of injury, SUDEP, and the social isolation that uncontrolled seizures create.
What Separates a Successful DBS Outcome from a Poor One
The deep brain stimulation success rate is not fixed. It is directly influenced by decisions made before, during, and after surgery. Understanding these factors is the most useful thing any patient or family can take from this article.
Patient Selection
This is the single biggest determinant of outcome. A Parkinson’s patient with significant dementia will not benefit from DBS regardless of surgical precision. A patient misdiagnosed with Parkinson’s who actually has a Parkinson’s-plus syndrome will not respond to STN stimulation. Correct diagnosis and careful candidacy evaluation at a specialist functional neurosurgery centre determine more of the outcome than any device or surgical technique.
Electrode Placement Accuracy
The subthalamic nucleus, the primary Parkinson’s DBS target, is approximately four millimetres wide. Electrode placement accuracy within one to two millimetres determines whether the patient walks better or experiences stimulation-related side effects. This is why surgeon experience in functional neurosurgery specifically, not general neurosurgery, matters.
Research published in a 2024 study in MDPI Biomedicines found that patients whose electrode field overlapped both the STN and the dentato-rubro-thalamic tract (DRTt) showed more than 50% improvement in UPDRS-III motor scores in most cases, with the distance from the electric field to the DRTt being the most robust predictor of clinical benefit.
Post-Operative Programming Quality
A perfectly placed electrode with suboptimal programming will produce suboptimal outcomes. Programming is not a one-visit process. It requires multiple sessions over three to twelve months, adjusting voltage, pulse width, and frequency across multiple electrode contacts. Patients who attend all programming sessions consistently reach better outcomes than those who drop out early or access programming from non-specialist centres.
Realistic Expectations and Compliance
Patients who understand what DBS does and does not do report higher satisfaction. DBS reduces symptoms. It does not stop disease progression, eliminate all medications, or provide an immediate cure. The patients who do best are those who enter surgery with clear expectations, attend follow-ups consistently, and give the programming process the six to twelve months it needs to reach its full potential.
“I tell every patient before surgery: the device gives you the hardware. Your follow-up gives you the outcome. I have seen patients with textbook electrode placement reach 80% motor improvement because they came to every programming session. I have seen other patients with similarly good placement plateau at 40% because they stopped following up after three months. The surgery is half the story.”
Dr. Jaspreet Singh Randhawa
DBS Success Rate in India: Is It Different from Global Standards?
At experienced functional neurosurgery centres in India, DBS outcomes are comparable to published global data. The devices are identical: the same Medtronic, Abbott, and Boston Scientific systems used in the USA and Europe. The surgical techniques follow the same internationally established protocols.
What differs is access. In the USA and UK, patients may wait twelve to eighteen months for DBS evaluation and surgery. In India at a specialist centre like Medisyn Neuro Centre, Mohali, the evaluation-to-surgery timeline runs four to eight weeks for confirmed candidates.
For international patients, this speed advantage combined with the cost difference (Rs.13 lakh to Rs.27 lakh versus $60,000 to $100,000 in the USA) makes India a compelling destination without any compromise on outcome quality.
According to long-term data reviewed on PubMed covering 320 Parkinson’s patients followed for up to 13 years, tremor responded best to DBS at 72.5% improvement, with other motor symptoms remaining stable over the long term. The Parkinson’s Foundation confirms that DBS success is strongly tied to the experience of the evaluating team and the quality of post-surgical programming.
If you or a family member is considering DBS surgery and want an honest evaluation of whether the procedure is appropriate for your specific condition and stage, Dr. Jaspreet Singh Randhawa at Medisyn Neuro Centre provides specialist functional neurosurgery consultations. Book an appointment to begin that conversation with the right information in hand.