You wake up with it.
Why do I have headaches everyday, you ask yourself. Or why do I get headaches everyday when nothing obvious has changed. Or simply, why does my head hurt everyday, again.
Or it arrives by 11am without warning.
Or it sits quietly in the background all day, never fully going away, never quite becoming unbearable.
If you are asking why do I always have a headache, you are describing something that has become part of your daily routine. Not a dramatic, lying-in-the-dark migraine. Just a persistent, grinding, always-there head pain that nobody has given you a proper answer about.
That answer exists. And it is usually specific.
Dr. Jaspreet Singh Randhawa, neurosurgeon at Medisyn Neuro Centre in Mohali, has evaluated thousands of patients with exactly this complaint. His observation is consistent: when someone always has a headache, there is almost always a diagnosable cause. Usually more than one, working together.
This article works through the 5 most common causes, shows you how to identify which one fits your pattern, and gives you Dr. Randhawa’s clinical perspective on what most people who always have a headache are actually missing.
Before the Causes: One Question That Changes Everything
Is there any time of day when your head feels completely normal?
Even 30 minutes?
If yes, you have a high-frequency daily headache with brief relief windows. If no, if your head never fully clears, you are looking at a different clinical picture, covered in detail in the article on constant headaches.
For everyone who gets at least a few pain-free minutes per day, the 5 causes below cover nearly every case.
Cause 1: You Have Been Running on the Wrong Amount of Sleep for Too Long

Sleep is where the brain resets its pain threshold.
When you consistently sleep fewer than 6 hours, or when your sleep and wake times are irregular, that reset does not happen properly. Chemicals that lower your sensitivity to pain do not clear. Chemicals that raise it build up overnight. You wake up with a headache because your nervous system is already running in a sensitised state before the day even starts.
This is not about one bad night.
It is about the cumulative effect of weeks or months of inadequate sleep. Most people who always have a headache and sleep fewer than 6 hours a night do not connect the two, because the headache feels like the problem, not the symptom.
Does your headache get worse on days when you slept poorly the night before?
If yes, sleep is almost certainly a major driver. The fix is not a sleeping tablet. It is consistent sleep and wake times, including weekends, maintained for at least 4 to 6 weeks before expecting a change in headache frequency.
“One of the most common things I hear is, ‘I slept 8 hours but still woke up with a headache.’ When I ask further, it turns out they slept at 1am and woke at 9am. The duration was fine, but the circadian timing was off. The brain’s pain regulation is tied to the clock, not just the total hours.”
Dr. Jaspreet Singh Randhawa, Medisyn Neuro Centre, Mohali
Sleep apnea is a specific and frequently missed cause of morning headaches that is entirely separate from sleep duration. If your morning headache clears within 30 minutes of getting up and moving around, and you snore or feel unrefreshed despite 7 or 8 hours in bed, sleep apnea needs to be ruled out with a sleep study.
Cause 2: The Painkiller in Your Drawer Is Sustaining the Headache

This is the one cause most people with a daily headache have never heard about.
When you take a painkiller, it works. The headache reduces. A few hours later, it comes back. So you take another one. This happens every day.
Over weeks and months, the brain adapts. It begins to expect the medication. When the drug level in your bloodstream drops, the brain reads this as a signal to produce pain. The headache is no longer being caused by the original trigger. It is being caused by the medication itself.
This is called medication overuse headache. And it affects:
- Paracetamol users taking it 15 or more days per month
- Ibuprofen or aspirin users taking it 15 or more days per month
- Combination tablet users (those containing caffeine) on 10 or more days per month
- Triptan users for migraine on 10 or more days per month
Does your headache come back a few hours after the tablet wears off?
That is not the original headache returning. That is rebound. The cycle needs to be broken under neurological supervision, because stopping abruptly typically causes 3 to 7 days of intensified headache before the brain recalibrates.
“A patient came to me recently who had been taking Dolo 650 every day for 9 months. She told me painkillers were the only thing that worked. I had to explain that the painkillers had long stopped working, they were simply preventing the withdrawal headache from peaking. Her actual headache, the one she had before all this started, was a mild tension headache. Medication overuse had transformed it into a daily constant.”
Dr. Jaspreet Singh Randhawa
The 2024 Delhi NCR headache study found a 3% prevalence of medication overuse headache in North India. Women are 5.1 times more likely to develop it than men. For a significant number of patients, “Why Do I Always Have a Headache?” begins with regular painkiller use that slowly turns occasional headaches into a daily pattern. That 3% figure translates to tens of millions of people in India alone who always have a headache because the solution they found made it permanent.
For the full picture of how this develops and how it is treated, see the article on daily headache causes.
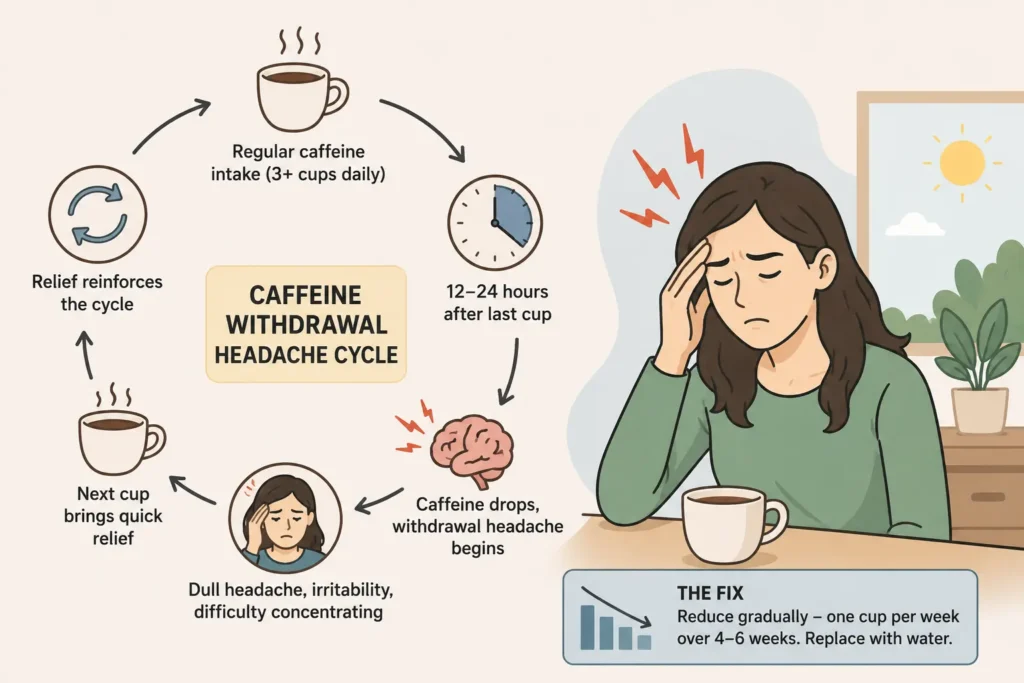
Cause 3: Your Body Is Running on Caffeine and Calling the Withdrawal a Headache
This one is simple. And very common.
If you drink 3 or more cups of tea or coffee daily, your brain has adapted to that caffeine level. The moment your blood caffeine drops below the threshold, usually 12 to 24 hours after your last cup, a withdrawal headache begins.
It feels like pressure across both sides of the head. It is dull and persistent. It comes with mild irritability and difficulty concentrating. And it relieves remarkably fast with your next cup, which reinforces exactly why you keep drinking it.
Does your morning headache clear within 20 minutes of your first tea or coffee?
That is caffeine withdrawal. Every morning. It is predictable, reproducible, and entirely self-inflicted.
The fix is not to stop caffeine suddenly. That makes the withdrawal headache significantly worse for several days. The fix is a gradual reduction of one cup per week over 4 to 6 weeks, replacing the reduced dose with water.
“My personal opinion on caffeine and headaches: I do not tell patients to stop tea or coffee. I tell them to stop letting caffeine make decisions for them. If you cannot function before your morning chai, that is not a preference. That is a dependence. The headache is the bill.”
– Dr. Jaspreet Singh Randhawa
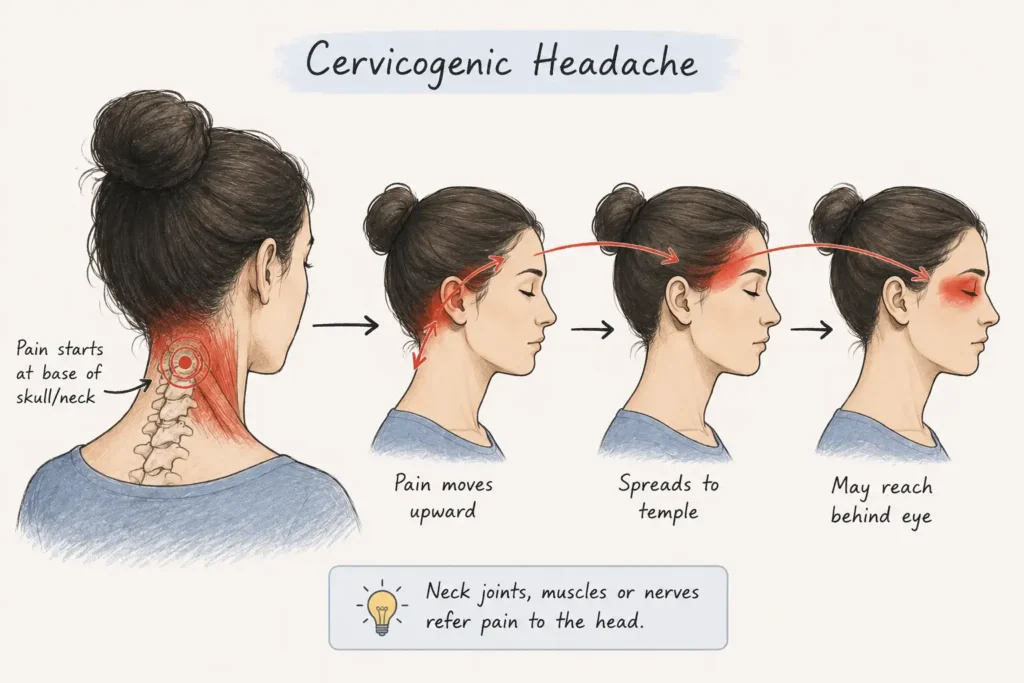
Cause 4: Your Neck Is the Origin, Not Your Head
A cervicogenic headache originates in the joints, muscles, or nerves of the cervical spine and refers pain to the head.
Most people do not feel the neck as the source. They feel it as a headache at the back of the skull, across the temple, or behind one eye. The neck feels slightly stiff, but the dominant complaint is head pain, so that is what gets treated. And because the neck is never addressed, the headache keeps coming every day.
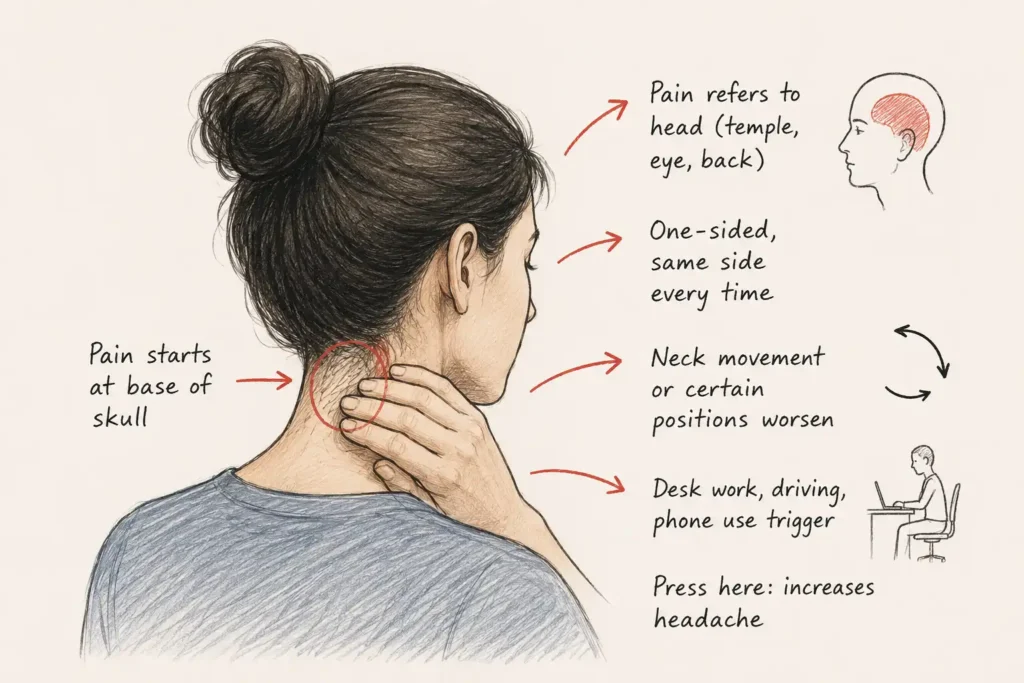
The pattern that identifies a cervicogenic headache:
- Pain usually starts at the base of the skull and moves forward
- It is almost always one-sided, on the same side every time
- Turning the head, looking up, or sleeping in certain positions worsens it
- Sustained desk work, driving, or looking at a phone for extended periods consistently brings it on
- Standard headache medication provides only partial, temporary relief
Does pressing on the back of your neck, just below the skull, reproduce or worsen your headache?
That is a highly specific test for cervicogenic origin. It is not definitive, but it is a very reliable indicator that the neck is involved.
Cervicogenic headache does not respond well to painkillers because the cause is mechanical. Targeted physiotherapy, cervical joint mobilisation, and postural correction produce lasting improvement where medications produce only temporary suppression.
You can read more about how to tell whether your headache is cervicogenic or migrainous in the article on migraine vs headache.
Cause 5: You Have an Unaddressed Migraine Condition
Migraine is not just a severe headache.
It is a neurological condition of heightened brain sensitivity that, when undertreated, transitions from episodic attacks to a near-daily background pain. This is called chronic migraine, and it is defined as headache on 15 or more days per month with at least 8 of those days having clear migraine features.
The background daily headache of chronic migraine is often dull and unremarkable. Patients describe it as just always being there. The classic, dramatic migraine attacks with throbbing and nausea happen on top of it, a few times a week or month.
Most people focus on treating the dramatic attacks and ignore the daily background. But the background is the condition signalling that the migraine threshold has lowered to the point where the brain is nearly always sensitised.
Do you have occasional severe, one-sided, throbbing headaches with nausea or light sensitivity, on top of a daily milder headache?
That combination is chronic migraine until proven otherwise.
The treatment is preventive medication taken daily, not just acute treatment for the bad attacks. Preventive medication for migraine is not a painkiller. It is a neurological agent that raises the brain’s pain threshold over 3 to 6 months, reducing both the severe attacks and the daily background.
“I see patients who have been managing migraine for 10 or 15 years with triptans alone. Triptans work brilliantly for an acute attack. But if someone is having attacks 8 or more times a month and taking triptans each time, they are accelerating the transition to chronic migraine and building a case for medication overuse headache simultaneously. Preventive treatment should have been started years earlier.”
– Dr. Jaspreet Singh Randhawa, Medisyn Neuro Centre, Mohali
For women whose daily headaches are linked to their cycle, PCOD, or perimenopause, the article on female daily headache causes addresses the hormonal dimension of chronic migraine specifically.
Dr. Randhawa’s Clinical Pattern: What He Hears Most Often
When patients come to Medisyn with a complaint of always having a headache, there is a pattern Dr. Jaspreet Singh Randhawa sees repeatedly.
It almost never turns out to be just one cause.
The typical presentation looks like this:
- A real, underlying headache type (tension or migraine) that was never properly diagnosed
- Caffeine dependence that adds a withdrawal layer every morning
- Painkiller use that is now frequent enough to create a rebound component
- Poor or irregular sleep that keeps the pain threshold low
“When I list these out on paper for a patient, I can see the moment it clicks for them. They have been treating each component as if it was the whole problem, when really there were four things feeding into each other. You cannot fix medication overuse while caffeine dependence is still running. You cannot fix cervicogenic headache while the patient is sleeping 5 hours a night. These causes have to be unwound in the right sequence.”
Dr. Jaspreet Singh Randhawa
Find Your Pattern: Which Cause Fits You
| Your Headache Pattern | Most Likely Cause | First Step |
|---|---|---|
| Worst on waking, improves after tablet, returns as tablet wears off | Medication overuse headache | Count your tablet days per month honestly |
| Clears within 20 min of first tea or coffee | Caffeine withdrawal | Gradual caffeine reduction over 4 to 6 weeks |
| Starts at base of skull, one-sided, worse with neck movement | Cervicogenic headache | Physiotherapy assessment |
| Always there, with occasional severe throbbing attacks | Chronic migraine | Neurological evaluation for preventive treatment |
| Worst after poor sleep, improves after a good night | Sleep-driven headache | Consistent sleep schedule for 6 weeks |
| Morning headache, snoring, unrefreshed sleep | Sleep apnea | Sleep study |
| Does not fit any of the above | Needs clinical assessment | See Dr. Randhawa at Medisyn Mohali |
When Always Having a Headache Needs Urgent Attention
Most daily headaches that have been present for weeks or months are not dangerous.
But these features change that assessment immediately:
- The headache is getting progressively worse every week with no plateau
- It wakes you from sleep at a consistent time each night
- It is accompanied by any neurological symptom: weakness, vision change, speech difficulty
- It started after a head injury
- You are over 50 and this headache pattern is entirely new
Any of these features means the headache needs imaging and a neurological examination before a primary diagnosis is assigned. Not because something is definitely wrong. Because these features make a secondary cause plausible enough that it cannot be assumed away.
According to Mayo Clinic, the vast majority of daily headaches are primary disorders: tension, migraine, and medication overuse. But secondary causes including intracranial lesions, CSF pressure disorders, and vascular abnormalities present with the same complaint. Clinical evaluation is the only reliable way to distinguish them.
Dr. Jaspreet Singh Randhawa evaluates patients with daily and persistent headache at Medisyn Neuro Centre in Mohali. The evaluation is structured, the diagnosis is specific, and the treatment is cause-matched rather than generic.
For patients whose headaches come with associated neurological symptoms such as dizziness, memory changes, or episodic weakness, the stroke and vascular neurology page at Medisyn explains when those features need urgent vascular investigation.
According to 2024 Delhi NCR study, fewer than 25% of people with chronic headache in India had engaged with a healthcare provider about it in the past year. Most were self-medicating. Most were making the underlying cause worse in the process.
10 Questions People Ask When They Always Have a Headache
1. Why do I always have a headache no matter what I do?
Because there is an underlying cause that has not been identified and addressed. Headaches that persist regardless of rest, hydration, or over-the-counter medication almost always involve either medication overuse headache, chronic migraine, an unresolved sleep issue, or a cervicogenic origin. None of these resolve on their own without targeted intervention.
2. Why do I get headaches everyday even when I am not stressed?
Stress is one trigger among many. Medication overuse, caffeine dependence, poor sleep timing, and cervicogenic dysfunction all produce daily headaches independently of emotional state. If stress reduction alone has not helped after 4 weeks, something else is driving the headache and it needs to be found.
3. Why does my head hurt everyday at the same time?
Timing is one of the most useful diagnostic clues in headache medicine. Morning headaches point toward sleep apnea, medication overuse, or caffeine withdrawal. Afternoon headaches point toward screen fatigue, caffeine wearing off, or skipped meals. Evening headaches point toward accumulated muscle tension and stress decompression. Same-time-every-day headaches are almost always linked to a recurring daily trigger that occurs at the same point in your routine.
4. Is it normal to have a headache every single day?
No. Common, but not normal. A headache on 15 or more days per month for 3 or more months is classified medically as chronic daily headache. It has specific causes and specific treatments. Accepting daily head pain as normal and managing it with tablets is the most reliable way to develop medication overuse headache on top of the original problem.
5. Why do I have a headache everyday when I wake up?
Four causes produce morning headaches specifically: sleep apnea (oxygen drops overnight cause vasodilation and head pain), medication overuse (analgesic blood levels drop overnight, brain responds with pain), caffeine withdrawal (if heavily caffeine-dependent, the overnight gap is long enough to trigger withdrawal), and bruxism (jaw clenching during sleep creates sustained temple and jaw muscle tension). Each has a different evaluation and treatment pathway.
6. Why do I get headaches every day after looking at screens?
Extended screen use causes two distinct problems simultaneously. First, eye strain from sustained near-focus and reduced blink rate causes direct eye fatigue that refers pain around the eyes and forehead. Second, sustained forward head posture with the chin protruding toward the screen loads the cervical joints and muscles, producing cervicogenic pain that radiates to the back of the skull and temples. The 20-20-20 rule helps with the eye component. Postural correction with physiotherapy addresses the cervical component.
7. Can anxiety cause daily headaches?
Yes, through two mechanisms. First, anxiety maintains chronic muscle tension in the head, neck, and shoulders that produces tension-type headaches. Second, anxiety is associated with disrupted sleep, irregular eating, and increased caffeine consumption, all of which independently drive daily headaches. Treating anxiety alone often significantly reduces headache frequency, but the physical components such as posture and sleep regularisation still need to be addressed alongside it.
8. Why do I always have a headache but no other symptoms?
The majority of primary headache disorders, including chronic tension headache, medication overuse headache, and the background component of chronic migraine, present as isolated daily head pain with no other features. The absence of additional symptoms is reassuring but does not eliminate the need for a diagnosis, since each of these conditions has a different treatment approach and self-treating all of them the same way is what typically makes them worse over time.
9. What could be the cause of daily headaches that have been there for months?
The most likely causes in order of clinical frequency are: medication overuse headache, chronic tension-type headache, chronic migraine, cervicogenic headache, and sleep-related headache. A secondary cause such as an underlying medical condition becomes increasingly worth excluding when the headache has been present daily for more than 3 months without improvement. This is the threshold at which a neurological evaluation is strongly recommended rather than optional.
10. When should I see Dr. Jaspreet Singh Randhawa in Mohali for daily headaches?
Book an appointment at Medisyn if your headache occurs most days of the week, if you have been taking painkillers more than 10 days per month for more than a month, if the headaches are interfering with your work or daily function, or if any of the 5 warning features listed above apply. Daily headaches are among the most treatable chronic conditions in neurology when properly diagnosed. They are among the most persistent when mismanaged.