One in four adults in India has experienced a migraine attack in the past year. That figure comes from population studies conducted across the country, and it is striking not because of its size alone, but because of what follows it: fewer than one in four of those people ever seeks medical help. Most reach for a strip of paracetamol, lie down in a dark room, and wait it out. For a large number of them, this approach works well enough. But for a meaningful number, the headache is not just a headache, and waiting it out is exactly the wrong decision.
The question every person in Mohali, Kharar, or Chandigarh who has ever had a severe, recurring, or unusual headache should be asking is not “which tablet should I take?” The question is: what kind of headache is this, and does it need a specialist?
This article will walk you through the real difference between a regular headache and a migraine, help you recognize when your head pain is a neurological red flag, and explain precisely when seeing a migraine specialist in Mohali changes your outcome. The information here comes from clinical practice, not from generic health websites. It is written to help you make a more informed decision about your own health.
Why Most People in Punjab Get the Diagnosis Wrong
Walk into any medical shop in Kharar or Sector 70 in Mohali and ask the pharmacist for something for a “migraine.” You will likely walk out with a combination painkiller. The pharmacist is not wrong to hand it over, but the problem is that many people using the word “migraine” are actually describing a tension headache, a sinus headache, or even a blood pressure headache. The reverse is equally common: someone dismissing a genuine migraine as “just stress” for years, while their condition silently worsens.
The confusion is understandable. All of these headaches hurt. But they have different origins, different warning signs, and importantly, different treatment paths. Getting the diagnosis wrong means taking the wrong treatment, and in some cases, it means missing something far more serious.

Regular Headache vs Migraine: The Clinical Difference That Actually Matters
A regular tension-type headache typically presents as a dull, steady pressure that feels like a tight band around both sides of the head. It usually builds gradually, is moderate in intensity, and goes away within a few hours with rest or a standard painkiller. There is no nausea, no sensitivity to light, no visual disturbances. Most people can continue light activity through a tension headache.
A migraine is a neurological event. It involves abnormal brain activity that affects the nervous system, blood vessels in the brain, and sensory processing. Clinically, a migraine is diagnosed when a patient has recurring headache attacks with at least two of the following characteristics:
- Pain on one side of the head (though it can be on both sides in some types)
- Throbbing or pulsating quality rather than dull pressure
- Moderate to severe intensity that limits or prevents normal activity
- Worsens with routine physical activity like walking up stairs
And at least one of these associated symptoms:
- Nausea or vomiting
- Sensitivity to light (photophobia) and sound (phonophobia)
A migraine attack typically lasts between four hours and 72 hours without treatment. That is a very long time to be in pain, and it explains why people with untreated migraines often find themselves unable to work, care for children, or function normally during an attack.
What Is Migraine Aura and Why Does It Concern Neurologists?
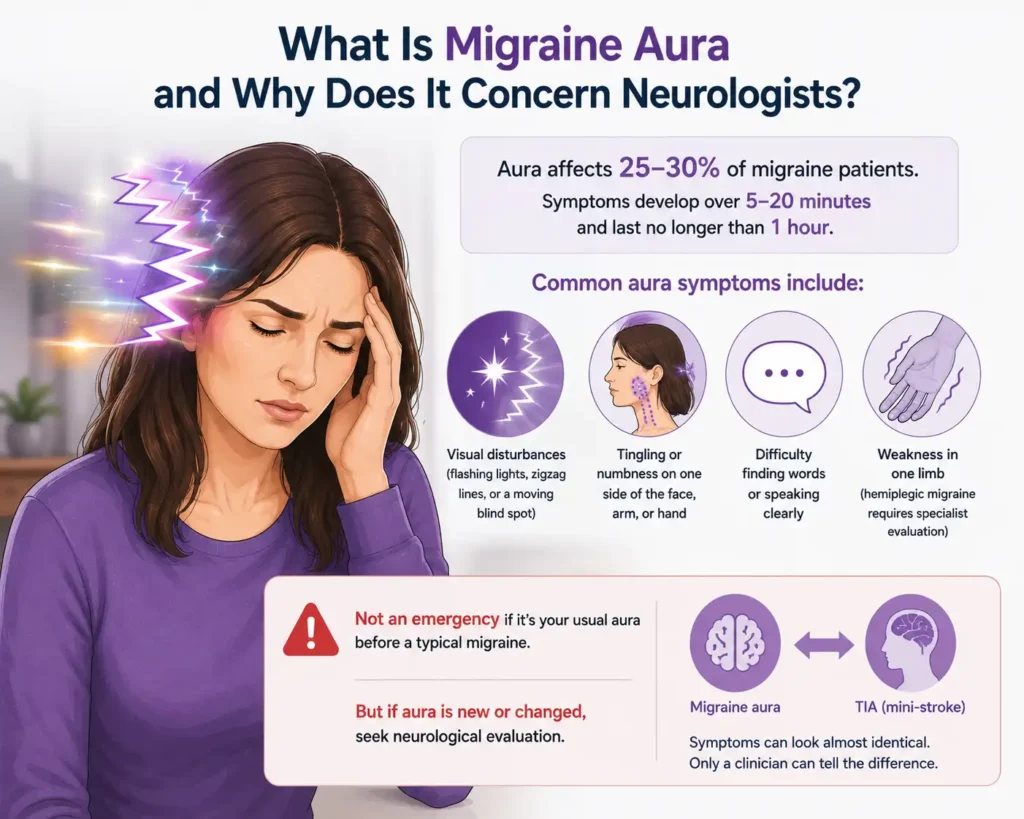
About 25 to 30 percent of migraine patients experience what is called an aura before or during the headache phase. An aura is a group of neurological symptoms that typically develop over five to twenty minutes and last no longer than an hour. Aura symptoms can include:
- Visual disturbances such as flashing lights, zigzag lines, or a blind spot that seems to move across the visual field
- Tingling or numbness in the face, arm, or hand, usually on one side
- Difficulty finding words or speaking clearly
- Weakness in one limb (this type, called hemiplegic migraine, requires specialist evaluation because it can mimic a stroke)
Aura on its own, when it occurs predictably before a migraine that follows the same pattern every time, is not a medical emergency. However, any patient experiencing aura symptoms for the first time, or aura that changes in character, needs neurological evaluation. The reason is simple: the symptoms of a migraine aura and a transient ischaemic attack (TIA, or “mini-stroke”) are almost identical. Only a clinician can tell them apart.
The Phases of a Migraine Attack Most Patients Don’t Know About
Most patients are aware of the headache phase, but a migraine actually moves through four distinct stages. Recognizing all of them can help a patient seek treatment earlier, before the pain becomes severe.
Prodrome begins up to 24 hours before the headache. During this phase, patients often notice mood changes, food cravings, neck stiffness, increased thirst or urination, frequent yawning, or unusual fatigue. Many patients in Mohali who later became regular patients at the clinic had been experiencing the prodrome phase for years without realizing it was connected to their migraines.
Aura follows in roughly one-third of patients, as described above.
Headache attack is the phase most people associate with migraine, characterized by severe, often one-sided pain that worsens with movement and is accompanied by nausea, vomiting, and sensory sensitivities.
Postdrome is the recovery phase that follows the headache, sometimes called the “migraine hangover.” Patients typically feel exhausted, mentally foggy, and mildly sensitive to light even after the pain has resolved. This phase can last a full day. Many patients find this phase as disabling as the headache itself.
Common Migraine Triggers That Are Especially Relevant in Punjab and North India
Migraine attacks are triggered by factors that vary from person to person, but there are patterns that appear frequently in patients from this region. Intense summer heat, particularly during May and June in Mohali, is a trigger for many patients who would not necessarily associate weather with their headaches. Long drives on the highway to Chandigarh, with exposure to strong sunlight and dehydration, frequently precede attacks in patients who commute for work.
Other common triggers include:
- Irregular sleep schedules, including sleeping significantly longer on weekends than on workdays
- Skipping meals, particularly in patients who fast for religious observances
- Strong smells, including incense, perfume, paint fumes, or vehicle exhaust
- Hormonal fluctuations in women, especially around menstruation, pregnancy, and perimenopause
- Excess caffeine consumption or, conversely, suddenly stopping caffeine after a period of high intake
- Emotional stress and anxiety, which are reported as triggers by the majority of migraine patients in clinical practice
- Bright or flickering lights, including tube lights with electrical flicker and extended screen time
Identifying personal triggers is a core part of migraine management. A headache diary, even a simple one maintained on a phone, is one of the most useful tools a patient can bring to their first specialist appointment. Recording the date, duration, intensity, associated symptoms, and any possible triggers for every attack gives the treating neurologist or neurosurgeon a clear diagnostic picture far faster than any scan.
When a Headache Is No Longer Just a Headache: Red Flags That Require Immediate Evaluation
This section is the most important in this article. The following symptoms, when present with a headache, are neurological red flags. They are not typical features of migraine. They may indicate a brain aneurysm, a haemorrhage, an infection of the brain lining, raised intracranial pressure, or a stroke. Any one of them warrants emergency evaluation, not a painkiller and rest.
- Thunderclap headache: A headache that reaches its maximum intensity within sixty seconds of onset, often described as “the worst headache of my life,” is a medical emergency until proven otherwise. This pattern is associated with subarachnoid haemorrhage (bleeding around the brain) and must be evaluated in an emergency setting immediately.
- Headache following a head injury: Any new or worsening headache that develops after trauma to the head, even seemingly minor trauma, requires neurological assessment. Intracranial bleeding can develop hours after the initial injury with no external signs.
- Headache with high fever, neck stiffness, or skin rash: These symptoms together raise concern for meningitis, an infection of the membranes covering the brain and spinal cord. This is a medical emergency.
- Headache with sudden vision changes, slurred speech, facial drooping, or one-sided weakness: These are stroke symptoms and require emergency evaluation. The F.A.S.T. acronym (Face drooping, Arm weakness, Speech difficulty, Time to call emergency services) applies here directly.
- Headache that consistently wakes you from sleep: Normal migraines do not typically wake a patient from deep sleep. A headache that reliably wakes you between 2 am and 4 am, particularly if it is accompanied by nausea or vomiting, may indicate raised intracranial pressure and needs investigation.
- New headache in a patient over 50: A first-ever significant headache in a person above the age of 50 requires neurological evaluation to exclude structural causes.
- Progressive headache worsening over weeks: A headache that steadily increases in frequency and severity over a period of weeks, rather than coming and going in attacks, suggests a structural or metabolic cause rather than primary migraine.
According to Cleveland Clinic, more than 40% of people will experience headaches severe enough to seek medical attention at some point in their lives. The challenge is knowing which of those headaches needs a specialist and which can be managed with lifestyle adjustments and standard medication. The red flags above are the clinical boundary between the two.
Who Should You See for a Headache in Mohali: GP, Neurologist, or Neurosurgeon?
This is a question that causes genuine confusion among patients in this region, and it is entirely understandable. Here is a straightforward guide.
A general physician is the right starting point for a new headache that does not meet any red flag criteria. They can rule out systemic causes (high blood pressure, thyroid disorders, anaemia, sinus infection) and provide initial management.
A neurologist specializes in the medical management of neurological conditions including chronic migraine, epilepsy, and Parkinson’s disease. If a GP suspects migraine and initial treatment is not effective, referral to a neurologist is the appropriate next step.
A neurosurgeon becomes relevant when imaging reveals a structural cause for the headaches, such as a brain tumour, an aneurysm, a malformation of blood vessels (AVM), hydrocephalus (excess fluid around the brain), or Chiari malformation. A neurosurgeon is also the appropriate specialist when a patient presents with any of the red flag symptoms described above. In a clinic like Medisyn in Kharar, Mohali, where both specialties are co-located, the patient benefits from a coordinated assessment that does not require a long referral journey across different hospitals in Chandigarh.
For a large number of patients, the visit to a neurosurgeon ends with a clean scan, a confirmed diagnosis of migraine, and a structured medication plan. That confirmation is itself valuable. Knowing that a recurring headache is not caused by a tumour or a vascular malformation removes enormous anxiety and allows the patient to focus on managing a chronic but non-dangerous condition.
Migraine Treatment Options: What Modern Medicine Actually Offers
The misconception that migraine is untreatable is one of the most damaging beliefs a patient can carry. There is no permanent cure for primary migraine, but there is excellent treatment for both the acute attacks and the long-term frequency and severity of episodes.
Acute migraine treatment is taken at the onset of an attack to stop or reduce its severity. This category includes triptans (sumatriptan, rizatriptan), which are migraine-specific medications that work by narrowing the blood vessels and blocking pain pathways in the brain. These are significantly more effective than over-the-counter painkillers for most migraine patients and are available by prescription. Anti-nausea medications are often used alongside them to address the nausea component of the attack.
Preventive migraine treatment is taken daily to reduce the frequency of attacks. Options include beta-blockers (propranolol), certain antidepressants (amitriptyline), anti-epileptic drugs (topiramate), and calcium channel blockers (flunarizine). The choice depends on the patient’s overall health profile, co-existing conditions, and specific migraine type. None of these are habit-forming when used appropriately under medical supervision.
Newer biological therapies, specifically monoclonal antibodies targeting the CGRP protein involved in migraine pain signalling, are now available in India. These are given as monthly or quarterly injections and have transformed outcomes for patients with chronic migraine (defined as 15 or more headache days per month). If you have chronic migraine that has not responded to standard preventive medications, this is a conversation worth having with a specialist.
Lifestyle-based management, including identifying and avoiding personal triggers, maintaining a consistent sleep schedule, staying well-hydrated, managing stress through structured relaxation techniques, and keeping a headache diary, forms the backbone of long-term migraine management alongside medication.
According to research published by the National Center for Biotechnology Information (NCBI), migraineurs in India lose an average of 5.8% of their productive time to headache attacks, and fewer than one in four seek healthcare. Effective treatment can dramatically reduce this burden.
A Note from Dr. Jaspreet Singh Randhawa, Neurosurgeon, Medisyn Neuro Centre, Mohali
“In my practice at Medisyn, I see a lot of patients who have spent years managing what they call their ‘headache problem’ on their own. Many of them have taken painkillers almost daily. What they don’t realize is that frequent use of over-the-counter painkillers, particularly combination drugs containing codeine or caffeine, can actually cause a separate type of headache called medication overuse headache. So the very thing they are using to control the pain is making it worse over time.
The other group of patients I see are those who delayed coming in because they were afraid of what a scan might find. My advice is always the same: a clean MRI scan is not a wasted visit. It is valuable information. It tells you what your headache is not, and that clarity gives you the confidence to manage it properly.
If you are in Mohali, Kharar, or Chandigarh and you have a headache that comes more than four times a month, lasts longer than a day, or has changed in character, do not wait. Come in, get evaluated, and start managing it with the right treatment rather than the nearest painkiller.”Dr. Jaspreet Singh Randhawa, MCh Neurosurgery (AFMC, Pune), Gold Medalist | Senior Neurosurgeon, Medisyn Neuro Centre, Mohali
How Medisyn Evaluates Headache Patients in Mohali
A new headache patient at Medisyn Neuro Centre in Kharar, Mohali typically goes through a structured assessment that begins with a thorough clinical history. The questions asked during this consultation are specific: How long have you been getting these headaches? Where exactly does the pain start and where does it spread? How long does each attack last? What were you doing when the headache began? Are you taking any medication for the pain, and how often? Have you noticed any visual disturbances, nausea, or neck stiffness? Is there a family history of migraines?
Based on the clinical history and a neurological examination, a decision is made about whether imaging is necessary. Not every headache patient needs an MRI. A straightforward migraine diagnosis in a young patient with a typical presentation and no red flags does not require a brain scan. Imaging is ordered when there is clinical uncertainty, when the headache pattern is unusual, or when red flag features are present.
If a scan is required, the MRI report is reviewed by Dr. Randhawa, and the findings are explained to the patient in plain language. Treatment is then customised. For migraine patients, this usually means a combination of acute medication, preventive medication if the attack frequency is high, and specific lifestyle guidance around the triggers identified during the consultation.
Patients who may benefit from a structured migraine treatment plan in Mohali are encouraged to book a consultation in advance, since wait times for a first appointment can be two to three days during busy periods. The clinic is located on Airport Road, Kharar, and is accessible from Chandigarh, Panchkula, Ropar, and most parts of SAS Nagar.
What Happens If a Headache Turns Out to Be Something More Serious?
If imaging or clinical examination points to a structural cause, the next steps depend entirely on the finding. A small unruptured brain aneurysm, for example, may be managed with watchful monitoring and blood pressure control rather than immediate surgery, depending on its size and location. A large or symptomatic aneurysm may require endovascular treatment or surgical clipping. A brain tumour found incidentally during a headache workup may be benign and slow-growing, requiring periodic monitoring, or it may require surgery depending on its characteristics.
The point is that finding something on imaging is not automatically catastrophic. It is information. Information that can be acted upon, planned for, and discussed with a specialist who has the training and experience to put it in clinical context. Dr. Randhawa’s training in complex neurosurgical procedures at AFMC Pune and his experience with operations at Healing Hospital Chandigarh and Medisyn Mohali means patients in North Punjab have access to a level of neurosurgical expertise that is typically found only in Delhi or Mumbai.
You can also learn more about related neurological conditions managed at the clinic, including brain stroke treatment in Mohali, where early evaluation plays an equally critical role in outcomes.
Practical Steps for Headache Patients in Mohali to Take Right Now
If you are reading this because you or someone close to you has been experiencing recurring or severe headaches, here are the concrete steps that will make the most difference.
Start a headache diary today. Note the date, start time, end time, pain location, intensity on a scale of one to ten, what you were doing before it started, what you ate in the six hours before, your sleep quality the previous night, and any associated symptoms. Two to three weeks of this data is more informative to a clinician than a year of “I just keep getting headaches.”
Stop taking over-the-counter painkillers more than ten to twelve days per month. If you are taking them more often than this, medication overuse headache may already be a factor in your pattern. A specialist can help you safely withdraw from this cycle.
See a doctor immediately, without waiting for a regular appointment, if any of the red flag symptoms described earlier in this article are present. The thunderclap headache, headache with fever and neck stiffness, and headache with stroke-like symptoms are emergencies. Go to a casualty department, not a clinic, for these.
For all other headache patterns that are recurring, worsening, or simply not responding to self-management, book a consultation with a neurosurgeon or neurologist in Mohali. The consultation itself will either give you a clear management plan or identify something that needs further attention. Either way, it is the right decision.
Frequently Asked Questions
1. What is the actual difference between a migraine and a bad headache?
A bad headache hurts, but it does not typically cause nausea, vomiting, light sensitivity, or visual disturbances. A migraine involves abnormal neurological activity in the brain that produces all of these symptoms together with the head pain. A migraine attack also lasts significantly longer, typically between four and 72 hours. The key distinguishing feature is not the intensity of the pain but the combination of symptoms and the duration.
2. Can migraine be permanently cured?
Primary migraine cannot be permanently cured, but it can be very effectively managed. With the right preventive medication, trigger avoidance, and lifestyle modifications, many patients reduce their attack frequency from ten to fifteen days per month to one or two. Newer CGRP-blocking medications have produced near-complete remission in some patients. The goal of treatment is not cure but significant, sustained reduction in the impact migraine has on your daily life.
3. My head pain is always on the right side. Does that mean it is a migraine?
Migraine is typically one-sided, so consistent right-sided or left-sided pain is consistent with migraine. However, consistent one-sided headache, particularly if it is new or worsening, should be evaluated by a specialist to rule out a structural cause on that side. One-sided headache by itself is not a red flag, but a new one-sided headache that is progressively worsening does warrant imaging.
4. How many times a month is too many headaches?
More than four migraine days per month is generally the threshold at which preventive treatment is recommended. More than fifteen headache days per month (regardless of type) meets the clinical definition of chronic daily headache and requires specialist management. If you are reaching for a painkiller more than twice a week for headaches, it is time to see a doctor.
5. Is it safe to take sumatriptan without a prescription in India?
Triptans like sumatriptan are prescription medications in India and should not be taken without a doctor’s evaluation. They are contraindicated in patients with certain cardiovascular conditions, uncontrolled hypertension, or a history of stroke. A proper prescription also ensures you are taking the right dose and combining it correctly with anti-nausea medication where needed.
6. I get visual disturbances before my headache. Should I be worried?
Visual disturbances that occur predictably before a headache that follows your usual migraine pattern are most likely a migraine aura and are not typically dangerous. However, visual disturbances that occur without a following headache, disturbances that last longer than an hour, or visual loss that does not fully recover need urgent evaluation. Any first-ever visual aura should be assessed by a specialist to confirm it is migraine-related and not a TIA.
7. Can stress really cause such severe headaches?
Stress is a well-established migraine trigger but is more precisely a trigger than a direct cause. Stress does not create migraine in someone who does not already have the neurological predisposition. For someone with migraine, however, physical or emotional stress can reliably provoke an attack. Managing stress through structured techniques (progressive muscle relaxation, regulated breathing, adequate sleep) is a legitimate and evidence-supported part of migraine management, not a substitute for medical treatment.
8. I had an MRI and it was normal. Why do I still get migraines?
A normal MRI is the expected finding in migraine. Primary migraine is a functional neurological condition, meaning it involves abnormal activity in normal brain tissue rather than a structural lesion. A clean MRI is not a failure of investigation; it is a positive finding that confirms the diagnosis is migraine and not something structural.
9. Which doctor should I see first for chronic headaches in Mohali?
If your headaches are recurring but do not involve any red flag symptoms, a general physician is a reasonable first step to rule out systemic causes. If the headaches are significantly impacting your quality of life, are not responding to initial treatment, or have features consistent with migraine, seeing a neurologist or neurosurgeon directly in Mohali is appropriate and will save you time. If you experience any red flag symptoms, go to a casualty department immediately.
10. Will I need surgery for my migraines?
The overwhelming majority of migraine patients do not need surgery. Surgery is relevant only if imaging reveals a structural cause for the headaches, such as an aneurysm, AVM, tumour, or Chiari malformation. For primary migraine, treatment is entirely medical and lifestyle-based. The neurosurgeon’s role in migraine management is primarily diagnostic, confirming that nothing structural is driving the symptoms and guiding medication management where needed.